
Pathology Case of the Month - Mexican Wolf
Case History: An eight-year-old male captive Mexican Wolf (Canis lupus baileyi) with clinical signs referrable to the central nervous system was euthanized by lethal injection in New York, USA. The wolf had been observed circling to the left, with proprioceptive deficits, knuckling of the right front foot, ataxia, and probable visual impairment.
Gross Findings: On external examination, a full complement of adult teeth was present. There was mild to moderate wear on all teeth with mild to moderate tartar accumulation, which was particularly marked on the carnassial teeth. The coat was in excellent condition. Two testes were present. There were no other significant findings.
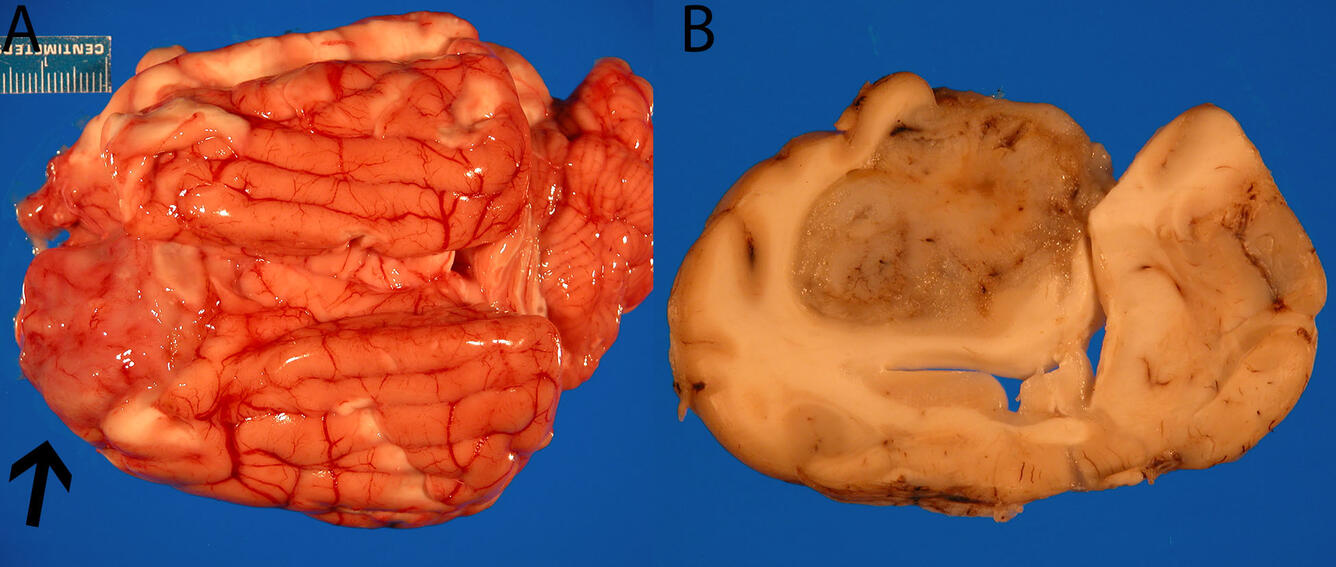
On internal examination, there was minimal subcutaneous fat and adequate visceral and epicardial fat. The spleen was engorged with blood (consistent with barbiturate euthanasia). The stomach was empty except for a small amount of grass, and the small intestine contained only scant amounts of soft tan digesta; formed feces were present in the colon. On examination of the brain, a 3 x 1 x 0.5 cm discrete area of light gray discoloration was present on the left cranio-dorsal surface of the cerebrum (Fig 1A). On cut surface, a large, expansile, irregularly lobulated, gray to tan, relatively well-demarcated mass with a jelly-like consistency was present within the dorsal medial cerebrum (Fig 1B). The mass was located primarily within the left cerebral hemisphere and compressed and displaced the dorsal portion of the right cerebral hemisphere.
Histopathological Findings: An unencapsulated, multifocally invasive, variably densely cellular neoplasm (tumor) is present in the cerebral cortex. The morphology of the tumor is variable. Most of the neoplastic tissue consists of loosely arranged, highly vacuolated stellate cells within a variably fine fibrovascular stroma (Fig 2A). Cell nuclei in these areas are small, round to ovoid, with densely packed chromatin and mild anisokaryosis. Multiple areas of necrosis, which are often surrounded by pseudopalisading cells, are present (Fig 2B), as well as foci of glomeruloid vascular proliferation (Fig 2C). The tumor is well-vascularized; blood vessels within areas of necrosis are often thrombosed; and there are occasional mild to moderate hemorrhages. In the parenchyma surrounding the tumor, there is variable reactive gliosis, and blood vessels often have swollen endothelial cells; a few are surrounded by small numbers of lymphocytes. In some areas, the line between tumor and brain parenchyma is blurred where tumor cells are invading the parenchyma in a pattern resembling gliomatosis cerebri.

Morphologic Diagnosis: Cerebrum: Glioblastoma multiforme
Disease: Glioblastoma multiforme (GM)
Etiology: The cause of this tumor in animals is unknown, and this is also true for most cases in humans, although exposure to ionizing radiation is a known risk factor. Rarely, it is associated with certain genetic abnormalities, such as neurofibromatosis type 1.
Distribution: GM is the most common primary brain tumor in humans. The incidence of this type of brain tumor in wolves is unknown, however, in dogs it is relatively rare, accounting for only about 5% of all astrocytomas.
Seasonality: Unknown/not applicable
Host range: Apart from humans, GM has mainly been documented in dogs, with brachycephalic species being overrepresented. Sporadic cases have also been reported in non-human primates.
Transmission: GM is a primary brain tumor and there is no evidence of transmissibility from one affected person/animal to another.
Clinical signs: Clinical findings are neurologic in nature and are dependent on the location of the tumor. GM most commonly occurs in the cerebrum but may rarely arise elsewhere in the central nervous system, including the spinal cord. Seizures, proprioceptive defects, and changes in mentation are the most commonly reported symptoms in dogs.
Pathology: In dogs, as in humans, GM arises mainly in the fronto-olfactory, temporal, and parietal regions of the cerebral hemispheres. Grossly these tumors are typically heterogeneous in appearance, with a mixture of yellowish necrotic areas, cystic foci, and areas of hemorrhage. Diverse histological features are also characteristic, with hallmarks of this tumor type including the presence of pseudopalisading around necrotic foci as well as foci of endothelial proliferation.
Diagnosis: Histopathologic examination of a biopsy or an excised mass is necessary for diagnosis.
Public health concerns: None when diagnosed in wildlife.
Wildlife population impacts: Unknown, but unlikely to be significant.
Management: Where possible, surgical removal is the treatment of choice. If complete resection is not possible, surgery may be followed by chemotherapy or radiation therapy. Prognosis is generally poor, as this is an aggressive malignant tumor; predicted survival time after diagnosis in humans is 12-18 months. Recently, however, a promising new treatment modality using intratumoral delivery of STING (stimulator of interferon genes) agonists in dogs has been described.
References:
- Boudreau CE, Najem H, Ott M, Horbinski C, Fang D, DeRay CM, Levine JM, Curran MA, Heimberger AB. 2021. Intratumoral delivery of STING agonist results in clinical responses in canine glioblastoma. Clin Cancer Res. 27:5528-5535. https://doi.org/10.1158/1078-0432.ccr-21-1914
- Hanif F, Muzaffar K, Perveen K, Malhi SM, Simjee ShU. 2017. Glioblastoma multiforme: A review of its epidemiology and pathogenesis through clinical presentation and treatment. Asian Pac J Cancer Prev. 18:3-9. https://doi.org/10.22034%2FAPJCP.2017.18.1.3
- José-López R, Gutierrez-Quintana R, de la Fuente C, et al. 2021. Clinical features, diagnosis, and survival analysis of dogs with glioma. J Vet Intern Med. 35:1902-1917. https://doi.org/10.1111/jvim.16199
- Porter BF, Summers BA, Leland MM, Hubbard GB. 2004. Glioblastoma multiforme in three baboons (Papio spp.). Vet. Path. 41:424-428. https://doi.org/10.1354/vp.41-4-424
- Urbańska K, Sokołowska J, Szmidt M, Sysa P. 2014. Glioblastoma multiforme – an overview. Contemporary Oncology/Współczesna Onkologia. 18:307-312. https://doi.org/10.5114%2Fwo.2014.40559
Related

WHISPers

Pathology Case of the Month

Diagnostic Services
Related
WHISPers
Pathology Case of the Month